Diabetic foot
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
26 NOVEMBER 2023
Patient came to causality with complaints of
Fever since 5 days
SOB since 5 days
Vomiting for 3 days
The patient was apparently asymptomatic 5 days back then he developed fever, high grade, not relieved with medication , associated with chills and rigors.
SOB since 5 days, grade III , no orthopnea , pnd.
Also presents with vomitings since 3 days, non bilious, non blood stained , watery, 2-3 episodes.
Ulcer over left foot,since 4 months, associated with edema of foot,
H/o abscess drainage???
New bleb notes since 2 days.
K/C/O DM II since 14 years, on Metformin 500 mg and Glimiperide 1 mg BD
K/C/O Hypertension since 20 yeats , on Amlodipine 5 mg.
Patient is a vegetarian since childhood.
No addictions
No allergies
Sleep adequate
Regular Bowel and bladder
Decreased appetite
Family history-
Both of the parents mother and father had diabetes.
Father was on medication.



Edema + left foot
Upto ankle
Vitals
Afebrile
BP - 80/60 mm Hg
PR- 104 bpm
RR- 18 cpm
Systemic examination
CVS- S1 S2 +
RS- BAE+
CNS- NFND
P/A - Soft, Non tender
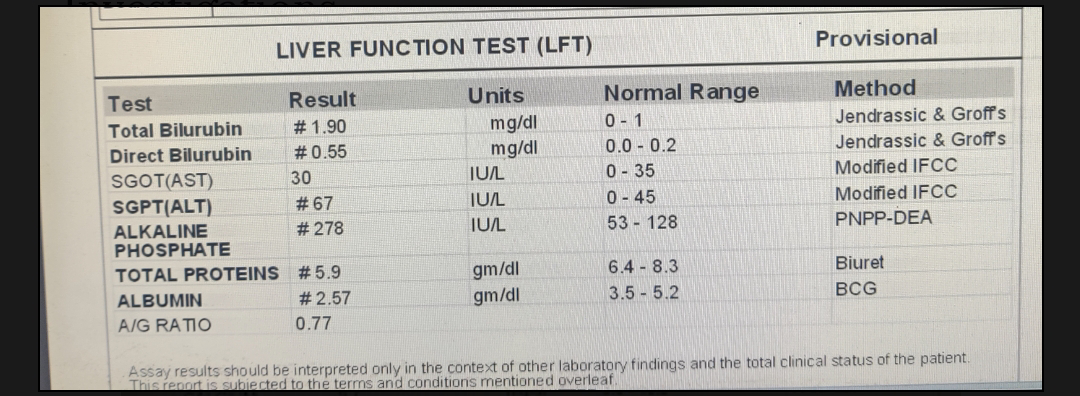
Investigations
Rbs- 311 mg/dl

 OSCE
OSCE

Comments
Post a Comment